














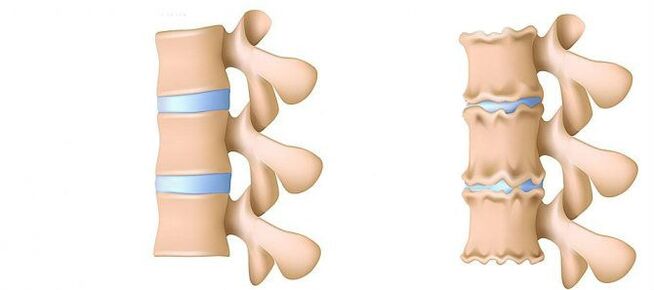
Osteochondrosis in the waist area is a disease that deforms and destroys the cartilage tissue of the lower back disc.Without the cartilage layer, the distance between the vertebrae will be significantly reduced.With a slight sharp turn, they can move.The main danger of this disease is the possibility of vertebral hernia.
Can't you lean over and raise an object that falls on the floor?Are you in lumbar spine with acute pain and walking regularly, wrapping your waist in a warm scarf?Don't ignore the conditions that bother you.
Osteocartilage in the waist area can be delayed for a long time.No need to experience the strength of the body.Love your body.It will pay off.
The majority of the weight load in the waist area compared to the chest and cervical departments.Therefore, this subspecies of osteochondrosis are the most common.
What is the development stage of osteochondrosis?
- The first stage.Prevent.The height of the disc is reduced.In the annulus of fibrous fibrous (the outer layer of the disc from the cartilage fibers), a crack is formed.The waist muscles begin to get tired very quickly.You will feel some discomfort in your back.
- Stage 2.Metabolic processes in the core coat (the central part of the disc, composed of a cartilage jacket): its cells have died or been completely destroyed.The collagen structure of the fibrous annulus (protein structure based on connective tissue) is also disturbed.Local pain, one cannot cope with what he previously thought was very feasible.
- Stage 3.Complete destruction of the fibre ring.The adjacent vertebrae stops stable.Any uncomfortable position can cause pain.Due to the experience of nerve roots, away from the spinal cord, the limbs become more sensitive and fluid.
- Stage 4.The fabric of the intervertebral disc becomes delicate.The vertebrae may be found in the shell.The clinical description here depends on the individual physiology.
During sciatic nerve (ISHIAS), low back pain (low back pain) and pain are one of the most common complaints patients seek medical help.Since these symptoms are very common in the general population and their stable growth is also noted, the diagnosis and treatment of such patients will remain one of the main areas of activity in neurosurgery hospitals.Despite this pathology, surgical removal of the intervertebral disc (MPD) is required in only 10% of patients with clinical manifestations of the lumbar spine.Among the remaining patients, the best effects are conservative treatments, including medication, physical therapy exercise, treatments using physiotherapy methods, and restoration of previous daily physical exercises.
Disease stage
Degenerative nutritional processes most often begin with deterioration in shock absorption function of the intervertebral disc.
- Blood supply deteriorates to the disc.In adults, food for the disc is performed by diffusion: only blood is delivered to the vertebrae, and has been “infiltrated” onto the disc through them.In the best way, the disk powers the pump in a dynamic load (e.g., walking) because of the principle of the pump (flow of fluid after compression, nutrients and oxygen flow when load is removed).Therefore, nutrition of the intervertebral disc is difficult, especially in the conditions of a sedentary lifestyle (sexual dynamics).
- Changes in the pulp core.As the blood supply deteriorates, the supply of water, sugar and amino acids is disturbed.Therefore, the production of carbohydrates connecting water is affected.The core is dehydrated, and its structure deteriorates from a gel-like structure to fibers, springs and extinguishing lenses.This increases the load on the annulus and vertebrae, which are more likely to be blocked and injured.
- Changes in the annulus of the intervertebral disc.Due to flattening of the pulp pulpos, the increased load is located on the fiber disk ring.In the event of insufficient blood supply, the fibrous annulus loses strength.Instability in the spine occurs, which can lead to the formation of vertebrae hernia, the displacement of vertebrae, and damage to the spinal cord or nerve roots.
- Disk herniated.The formation of vertebral hernia.As the fibers of the annulus weaken, the pulp pulposus begins to protrude, for example, towards the spinal canal (disc herniation).Such a stunning person can further lead to the rupture of the fibrous annulus and the formation of hernia.Read more about the process of disc hernia formation in another article: “Effective treatment of disc hernia at home”.
- Spondylosis is the damage of the vertebrae joints (spine and spine), the growth of bone and the ossification of ligaments.With the formation of intervertebral disc hernia, damage to vertebrae joints, destructive changes in vertebrae (cartilage) and ligaments in osteochondria.
As osteochondrosis and complications develop, you have to resort to medications increasingly, increasing the dose.Due to side effects of the drug, this leads to high financial costs and further deterioration of health.
Usually, using an orthopedic corset of varying degrees of stiffness to fix a spine or friend, can supplement medication.
Surgical treatment is only reasonable in the clinically determined level of spinal cord cavity compression, which corresponds to confirming rupture of the annulus whereas the hernia of MPD "loss" enters the lumen of the vertebral canal [3-6].Usually, surgical treatment results for patients with disc herniation are disappointed by the doctor and the patient themselves.The method to establish an accurate diagnosis is magnetic resonance imaging (MRI).Due to claustrophobia (worry about enclosed space), it is impossible for a regular MRI to occur in about 10% of the population.In people in this category, so-called "Open" MRI can be used, however, to obtain corresponding image quality losses.Patients who have previously undergone surgery must undergo MRI and have contrast enhancements to define postoperative scar-in-disc changes with true hernia herniation changes in the disc.In patients suspected of hernia protruding with MPD, special diagnostic value can be obtained when the implementation of MRI is impossible, or the results obtained are informative, calculated, orthopedic (CT) bone marrow.
Typically, private diagnostic experts who interpret the findings exaggerate the extent of damage to disks because it is impossible to compare clinical data with tomography.Conclusions like "changes correspond to changes in patients' age" are almost impossible in the study protocol.Despite the improvements in neuroimaging technology, the responsibility for correct deception diagnosis remains on the clinician’s shoulders, because only he can compare clinical images with data obtained from tomography.The resolution of the cleavage increased slightly improved surgical treatment outcomes, but deviations in asymptomatic patients were detected.In recent years, significant progress has been made in the process of spinal degenerative-persistent lesions.Arthritis of the arched joint is common in the general population and is often found in middle-aged and elderly groups during the CT study.Degenerative changes in MPD are often detected (also often widely used), and MRI is a more specific method for its diagnosis.At the same time, obvious changes in MPD are not uncommon, and are not accompanied by rupture of the annulus, but are only manifested as a slight "prick" of the intervertebral disc into the cavity of the spinal canal or vertebral foramen.In some cases, the degeneration process that occurs in MPD can lead to damage to the fibrous annulus, which can lead to a portion of the lung nucleus migrating and compressing adjacent roots of the spinal cord.Assert that if you notice the pain in your legs, it will definitely invade the legs at the root of the spinal cord.The pain in the buttocks exposed to the back surface of the thigh can lead to degeneration of the MPD itself and the arched vertebral joints.For the real attack of ISHIALGIA caused by Koreshka compression of MPD hernia nerve, the pain radiates on the back surface of the thigh and on the back surface of the lower leg.Uncertain pain is limited to the hip or thigh area and is not distributed along the sciatic nerve, as well as bilateral pain (on the right and then on the left) that changes its localization in the grain area or hip, usually caused by transgender degeneration of the arched joint or MPD.The clinical manifestations of Koruska compression of MPD hernia may also be a concomitant pathology (e.g., knee arthritis).In patients with this pain, no matter which pathology is detected by tomography, surgical treatment will not have an appropriate effect.In other words, in patients with back pain clinics only, MPD hernia is removed even if the tomography is determined by the protrusion of MPD, even if the tomography (as usual).However, there are also patients with a typical case of obvious disability pain syndrome, and in studies conducted with highly perceptual scanners, compression at the spinal cord root has not been determined.Patients in this category are not suitable for surgical intervention because radiation symptoms are usually mild over time.
It is necessary to clearly imagine the mechanisms that lead to the development of MPD hernia in order to recommend the amount of allowed exercise to the patient rather than forgetting work activities.The force that causes the hernia protrusion is the result of the degenerate changes of MPD, and the vertical (height) reduction of the fibrous annulus and slurry nucleus.The spine fragment of MPD moves in 80% posterior direction while introducing into the intraluminal cavity of the spinal canal and the medial portion of the vertebral foramen.The displacement of hernia towards the midline of MPD is facilitated by the holding force of the longitudinal ligament.Up to 10% of hernia bursts locally and spread to the outer edge of the vertebrae (Foss filament hernia) or the spine of the cerebral spine from which it appears, thereby squeezing it.
During the process of important activities, dehydration and degenerative changes lead to a high loss of MPD.These pathological processes involve both the annulus of fibrous and the pulp pulposus.In general, in the context of annulus accompanied by degeneration, more obvious damage to the pulp pulposus only leads to loss of MPD height without its obvious gathering.With the main changes in the fibre annulus, the vertical force affecting the retained pulp pulposus is the derivative of its own weight and the muscles on the back. It acts on the side disk on the side, and exerts too much pressure on the remaining fragments of the pore nucleus to retain the fibre annulus.
The sum of these two forces leads to an increase in the centrifugal pressure of MPD, which, together with the stretching component acting on the fibrous annular fiber, can cause the rupture of its remaining slurry core and the rupture and fragmentation of the fragments.After the hernia is formed, the "redundant" fragment of the pulp pulposus is outside the fibrous annulus, and the structure of the MPD becomes stable again [2].Due to the forces affecting the core and fibrous annulus of MPD, they are balanced, and their vectors help further emanate the protrusion of the nuclear fragments, thus disappearing.In some cases, partial degenerative changes in the PURPOS core contribute to the formation of gases inside the MPD, and then exert excessive pressure on its remaining fragments.The formation of hernia is also accompanied by the gas formation process inside the disk.
Excessive and dramatic physical activity displayed on the patient's back, in the context of existing degenerative-spine-like lesions, is often just a trigger, which leads to detailed clinical images of compressed radiation syndrome, which are often misperceived by the patient themselves (e.g., the original patient of the waist-eicialialgia).Clinically, MPD hernia can exhibit reflex and compression syndrome.Syndrome is called compression, in which the hernia is pulled out above the protrusion, squeezed and deformed, and the blood vessels or spinal cord are compressed and deformed.Reflexes include syndromes caused by the effect of disc hernia on these structural receptors, mainly returning to the ends of the spinal nerve, which leads to the development of reflexes manifested by vasodilation, dystrophy, myosinous myopathy and complement disease.
As mentioned above, in only 10% of patients, surgical treatment of degenerative-nutritional lesions is recommended, and the remaining 90% respond well to conservative measures.The basic principles for using the latter are:
- Relieve pain syndrome;
- Restore the correct posture to maintain the fixed ability to change MPD;
- Eliminate muscle and tonic diseases;
- Restore blood circulation in the roots and spinal cord;
- Normalization of conductivity in nerve fibers;
- Eliminate changes in protein and spacing;
- Relocation of mental illness.
treat
Today, in the treatment of osteochondrosis and its complications, the following groups of drugs are used:
- Net-ore anti-inflammatory drugs (NSAIDS) - in the form of tablets or injectable drugs.These funds have the ability to reduce pain and reduce inflammatory activity.However, their effects won't last long - from a few hours to two to three days.So it has to take a long time - weeks, sometimes months.At the same time, these drugs have a negative impact on the mucosa of the gastrointestinal tract.Their long-term reception is full of gastritis, the development of ulcerative lesions.In addition, they may negatively affect the work of the kidneys, liver and contribute to the development of hypertension.And, at the same time, these funds don’t help clean up the disk from dead cells.Therefore, their use is just a way to relieve symptoms for a while, but it does not eliminate the main problem.
- ctepid (Gopmonal) anti-inflammatory drugs.Usually, they are used for severe and impenetrable pains such as hernia, radical inflammation, stone, etc.Gopmons has the ability to eliminate inflammation manifestations (due to the compression of the immune system) and relieves pain.But they also negatively affect the mucosal membranes of the stomach and intestines, promoting calcium leaching from the bones and inhibiting the production of its own republicans.And don't help clean the focus of dead cells.
- Papasmolics is a drug that affects muscles or nerves and causes skeletal muscles to relax.These mean it helps relieve muscle clips for a while, relieve pain and improve blood flow.But at the same time, they do not help clean tissue from dead cells.Therefore, they do not help cure osteochondrosis.
- Additional inhibitory effects - Introduce painkillers and sugar-toxins into the space between the solid cerebral skull and periosteum.Usually, it is used for intense pain - in the acute period of intra-vertebral hernia, with severe radiation inflammation, is isotropic.Depending on the composition, this injection helps relieve pain from hours to days.After the expiration date, the manifestations of the disease are returned because the process does not help restore metabolic processes in the intervertebral disc.Additionally, it can be dangerous when blood vessels and nerves are damaged.
Conservative treatments include various orthopedic effects on the spine (cort fixation, traction, manual treatment), physical therapy (therapeutic massage, physical therapy exercise, acupuncture, electrotherapy, mixing, mixing, various heating), paramafret brain, thyroid venom, goiter, incubation therapy and medication.The treatment of degenerative spine-nutritional lesions should be complex and phased.Generally, the general principle of conservative measures is the appointment of painkillers, nonsteroidal anti-inflammatory drugs (NSAIDs), muscle laxity and physical therapy.
The analgesic effect is achieved by appointing diclofenac, ketoprofen, lonoxicam, and tramadol.The obvious analgesic and anti-inflammatory effects have lorox, present in injection and tablet form.
NSAIDS is the most widely used drug that causes damage to spinal degeneration.They have anti-inflammatory, analgesic and anti-dye effects associated with inhibition of cyclooxygenases (COC-1 and TSOS-2), which regulates the conversion of arachnoid acid to prostaglandin, prostaglandin, prostate cassette, and movable gun cassette.In older people and patients with risk factors for side effects, it is recommended to perform a “covering” of stomach meat under “cover”.In such patients, it is recommended to use a tablet form of COO-2 inhibitor with lower gastrointestinal side effects during injection therapy with NSAID.
To eliminate pain associated with increased muscle tone, it is recommended to include a central muscle agent in complex treatments.
Surgical treatment of spinal degenerative-hybrid lesions is reasonable for patients with hernia with MPD (usually more than 10 mm) and patients with non-scattered radiation symptoms.There is an emergency indication of the compression of secestra "falling" in the lumen of the spinal cord duct and the compression of the spinal cord root expression.The development of acute radioactive syndrome promotes acute radiationemia, which leads to severe hemoalgae syndrome, and even prescribed for drug analgesics, the use of blockade (glucocorticoids and anesthesia) does not reduce the severity of the pain.It is important to note that the absolute size of the disc hernia has no definite value for the final decision of surgical intervention. It should be related to the clinical situation and found through lamination examination.In 95% of cases, open channels of the spinal canal are used in hernia.Various steering wheel technologies (cold - plasma coagulation, laser reconstruction, etc.) have not been used yet, and their use is only suitable for protrusions of MPD.Classic open microsurgery to remove hernia from intervertebral discs is performed using microsurgery tools, binocular magnifying glass or operating microscope.Distant treatment results (within more than 2 years) of MPD hernia were analyzed, 6135 of which were removed, 7224 of whom were isolated and 7224 were subjected to quarantine and 7224 aggressive disc surgery, indicating that recurrence of pain was more common in 2.5 times (27.8% of patients), while patients in pain were more likely to suffer from 27.8% of the pain, while the number of pain in pain was higher than two times.(7% vs. 3.5%) Only isolated patients were removed.Patients with pain syndrome have a lower quality of life, and repeated hernia formation does not always manifest clinically.
In short, I will again emphasize the need for thorough clinical examination and analysis of tomography in order to make the best decision on the strategy for selecting a specific patient.